Chung-Ying Tsai, MS1,2, Alicia M. Koontz, PhD, RET1,2
1Human Engineering Research Laboratories, Department of Veterans Affairs, Pittsburgh, PA
2Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA 15261
BACKGROUND
In order to maintain a high quality of life and independence, manual wheelchair users’ reliance on the upper limbs causes upper limb joints to wear faster or develop injuries from the overuse (Lal, 1998). Transfers are an essential activity in daily living for wheelchair users, such as transferring to bed and commode. In a recent survey about what was perceived to be the most important mobility activities among wheelchair users, three of the top ten were related to transfers (Fliess-Douer, Vanlandewijck, & Van Der Woude, 2012). In addition to their importance to daily living, transfers are physically demanding often eliciting pain in the upper limbs when performed. (Curtis et al., 1995; Dalyan, Cardenas, & Gerard, 1999) .
Research on the biomechanics of transfers provides useful insight into the movements and forces involved that may predispose wheelchair users to injuries. For instance, studies have shown that during transfers the combination of shoulder flexion, abduction, and internal rotation, combined with the vertical reaction forces used to support body weight likely narrows the subacromial space and impinges the structures within the joint, such as the rotator cuff tendons (Boninger et al., 2005; Gagnon et al., 2009) . The loading on each joint of upper extremities during transfers is larger than any other wheelchair related weight-bearing activity (Gagnon, Nadeau, Noreau, Dehail, & Piotte, 2008). However, these studies have presented the biomechanics for transfers between two surfaces of equal height. Few studies have looked at other kinds of transfers. Muscular activation and forces increase when the height of the target surface for transfer increases or decreases (Gagnon, Nadeau, Noreau, Dehail, & Gravel, 2008; Wang, Kim, Ford, & Ford, 1994) . The biomechanics of transfers to real surfaces encountered in daily life such as commodes, beds, car seats have not been researched.
Commode transfers present a unique set of challenges for wheelchair users. For instance they often take place in small and constrained spaces. Little room is available to position the wheelchair for the transfer. Also the height of the commode (43.18 to 48.26 cm or 17 to 19") is lower than the average wheelchair plus cushion seat to floor height (55.88 cm or 22" (Toro, Koontz, & Cooper, 2012)) requiring a non-level height transfer for most people. Also there may not be a good spot to position their hands or use a grab bar as they may be outside of someone's reach distance or too high to get the mechanical advantage needed (Toro, et al., 2012). These factors all may make transfers more strenuous (Boninger, et al., 2005).
PURPOSE
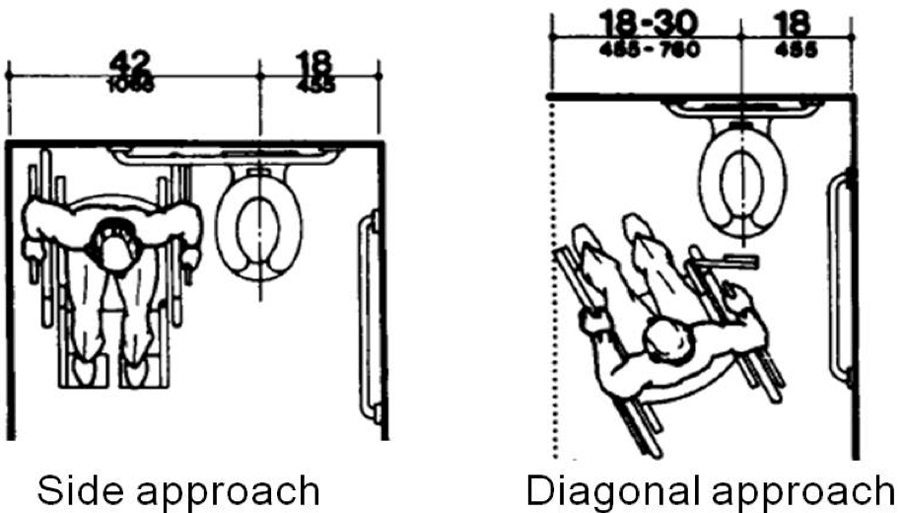 Figure 1: Two commode transfer approaches: side approach and diagonal approach("Americans with Disabilities Act (ADA) - Accessibility Guidelines for Buildings and Facilities,")
Figure 1: Two commode transfer approaches: side approach and diagonal approach("Americans with Disabilities Act (ADA) - Accessibility Guidelines for Buildings and Facilities,") The purpose of this study is to investigate upper limb and trunk movements (e.g. wrist, elbow, shoulder joints and trunk ranges of motion) when space limits how the wheelchair is positioned next to the commode. Based on the space available around the commode two general approaches will be possible: side or diagonal (Figure 1). ("Americans with Disabilities Act (ADA) - Accessibility Guidelines for Buildings and Facilities,") We hypothesized that the side approach would require less trunk rotation and upper limb joint range of motion. The findings of this study could help justify and potentially refine the clear floor space needed for performing biomechanically safe transfers around commodes as well as provide guidance on appropriate wheelchair approaches for commode transfers.
METHOD
Subjects
The study was approved by the Department of Veterans Affairs Institutional Review Board. The inclusion criteria of the study were: 1) have discernible neurological impairment affecting both lower extremities or transfemoral or transtibial amputation of both lower extremities; 2) at least one year post injury or diagnosis; 3) use a wheelchair for the majority of mobility (over 40 hours/week) 4) English speaking; 5) able to sit upright for at least 4 hours a day; 6) over the age of 18 years; 7) able to independently transfer to/from a wheelchair without human assistance or assistive devices. The exclusion criteria were: 1) current or recent history of pressure sores; 2) history of seizures or angina; 3) able to stand unsupported.
Experimental protocol
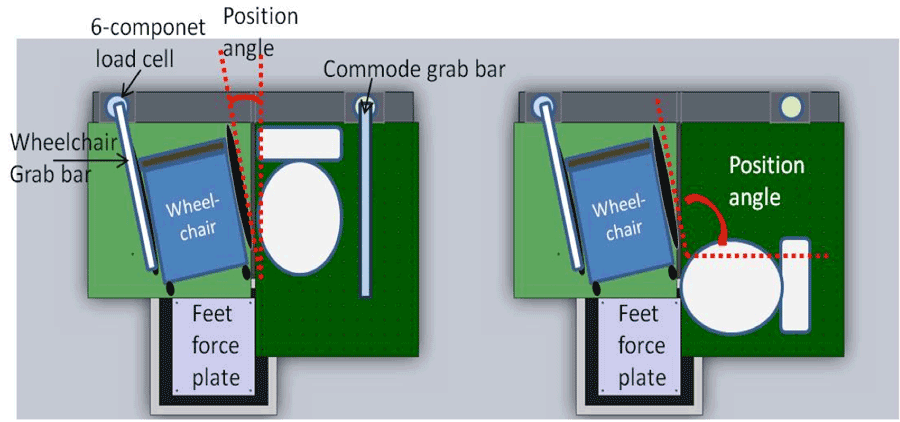 Figure 2: The transfer station setup for side (left) and diagonal (right) commode transfers.
Figure 2: The transfer station setup for side (left) and diagonal (right) commode transfers. After informed consent, subjects positioned their wheelchairs next to the commode on our transfer station (Figure 2) (Koontz, Lin, Kankipati, Boninger, & Cooper, 2011). The transfer station includes three force plates (Bertec Corporation, Columbus, OH) which are underneath the wheelchair, the commode, and the subject’s feet respectively, and two 6-component load cells (Model MC5 from AMTI, Watertown, MA; Model Omega 160 from ATI, Apex, NC) which are each attached to a steel beam used to simulate a armrest and grab bar. The transfer target and the subjects’ wheelchairs were secured to the aluminum platforms which cover the force plates. Reflective markers were placed on anatomical landmarks of the subjects’ trunk and upper extremities (Wu et al., 2005) . A ten-camera three-dimensional motion capture system (Vicon, Centennial, CO) was used to collect the marker positions during the transfers. To mimic the two transfer approach scenerios of Figure 1, we changed the orientation of the commode from facing forward to facing the wheelchair user (turned 90 degrees clockwise) (Figure 2). The grab bar on the commode side was only available for the side approach transfer due to mounting limitations of the station.
Subjects were asked to sit with their arms in an anatomical neutral position to collect a static trial of the marker positions first. After that, subjects were asked to perform the two commode transfers using their habitual approaches. They were free to adjust their wheelchair orientation in each case with respect to the commode within the confines of the space available on the platform [91.44 cm by 91.44 cm (3 feet by 3 feet)]. The angle and distance they positioned their wheelchair next to the commode was recorded (Figure 2). The angle was defined by the centerline of commode and wheelchair seat. The recorded distance is the shortest distance between the wheelchair and commode. The Subjects were restricted to moving to their left side from the wheelchair to the commode based on the setup. Also on the wheelchair side they needed to place their (trailing) hand on the steel beam so forces during the transfer could be recorded. Subjects performed up to five trials for each type of commode transfer. The order of the transfers was randomized. Subjects were given at least 10 minutes to rest between trials. Kinetic data from all the force plates and load cell were collected at 1000 Hz for the duration of each transfer. The kinematics data from all the cameras were collected at 100 Hz.
Data Analysis
A zero-lag low-pass Butterworth 4th order filter with a cut-off frequency of 7 Hz was used to filter the data. The vertical reaction forces from the load cell and the force plate underneath the commode were used to decide the beginning and the end of transfers. The transfer began when the load cell detected the hand force (rising from zero). The end of the transfer was the moment before the landing spike of the buttocks was detected by the commode side force plate (Kankipati, Koontz, Vega, & Lin, 2011). The independent variables are the two transfer approaches. The dependent variables in the study included peak angles and overall ranges of motion (ROM) of the leading (e.g. hand moving to new surface) and trailing (e.g. hand left on the old surface) wrists, elbows, shoulders and trunk during transfers from wheelchair to the commode. These variables were computed by Matlab (Mathworks, Inc., Natick, MA, USA) based on the rotation sequences which are recommended by International Society of Biomechanics (Wu, et al., 2005) and averaged values were determined over the five trials for each transfer approach. The Eular angle sequences for shoulder, elbow, and wrist were YXY, ZXY, and ZXY respectively. As for trunk, Cardan angle sequence, ZXY, with respect to the laboratory coordinate system was used.
Descriptive statistics (means and standard deviations) were calculated and reported for each variable. Each variable was averaged over a minimum of three and maximum of five trials. Because of the small sample size, non-parametric Wilcoxon signed-rank tests were used to compare differences between the two transfer approaches, and trailing and leading arms within each approach with a level of significance at p < 0.05. All the statistical analyses were performed in SPSS (SPSS Inc., Chicago, IL).
RESULTS
Six men volunteered to participate in the study. The group mean (±standard deviation) of age, height, and weight were 40.67 (±9.56) years, 67.5 (±2.74) inches, and 151.33 (±32.26) pounds, respectively. Their level of spinal cord injury (SCI) ranged from T2 to L1 with three having complete injuries and three with an incomplete SCI. The average duration (±standard deviation) of post-injury was 13.79 (±9.37) years.
For the side approach, the group mean (±standard deviation) of distance and angle between subjects’ wheelchair and the commode were 8.46 (±3.91) cm (range: 1.27~12.7 cm) and 30 (±14.83) degrees (range: 15~50 degrees). Two of the six subjects used the commode grab bar in our setup for the side approach. Others put their leading hand on the edge of the commode. As for the diagonal approach, the average distance and angle were 18.80 (±9.91) cm (range: 6.35~30.48 cm) and 108 (±9.08) degrees (range: 100~120 degrees). They all used the edge of commode as leading arm support.
The diagonal approach had larger maximal plane of elevation angle and ROM, maximal wrist extension and radial deviation angle and radial/ulnar deviation ROM in the trailing arm, as well as trunk extension/flexion and axial rotation ROM (p < 0.05) (Tables 1 and 2). The side approach had larger elbow flexion/extension ROM and extension movement in the trailing arm.
The trailing arm had larger elbow maximal flexion and flexion/extension ROM than the leading arm (p < 0.05). The leading arm had larger wrist radial deviation as well as wrist flexion/extension and ulnar/radial deviation ROMs.
|
Side approach (n=6) |
Diagonal approach (n=6) |
||
| Unit: Degree ( |
Trailing arm (Right) | Leading arm (Left) | Trailing arm (Right) | Leading arm (Left) |
Shoulder |
||||
| Max_POE 0°, abduction; 90°, flexion | 37.58* (±11.93) | 39.91† (±28.70) | 65.37* (±19.02) | 56.49† (±16.80) |
| Min_POE 0°, abduction; -90°, extension | -16.49 (±19.57) | -8.06 (±34.22) | -8.43 (±21.53) | -2.88 (±11.24) |
| Max_ELE | 56.62 (±17.40) | 60.29 (±19.55) | 57.33 (±24.10) | 61.49 (±16.50) |
| Min_ELE | 4.72 (±8.62) | 4.14 (±5.64) | 2.98 (±6.11) | 4.37 (±8.05) |
| Max_AXR IR(+)/ER(-) | 60.63 (±7.68) | 60.86 (±8.11) | 62.41 (±5.57) | 68.00 (±12.41) |
| Min_AXR IR(+)/ER(-) | 20.42 (±10.30) | 13.55 (±12.11) | 19.63 (±14.68) | 18.06 (±11.22) |
| Elbow | ||||
| Max_ FLEX(+)/EXT | 70.21 (±5.53) | 54.44 (±16.53) | 77.99¶ (±10.00) | 54.46¶ (±7.03) |
| Min_ FLEX(+)/EXT | 18.31* (±10.48) | 22.21 (±5.62) | 34.72*¶ (±3.84) | 18.98¶ (±6.03) |
| Wrist | ||||
| Max_ FLEX(+)/EXT | -16.14* (±16.59) | -3.58 (±18.70) | -24.17*¶ (±16.39) | -5.45¶ (±7.58) |
| Min_ FLEX(+)/EXT | -48.99* (±17.48) | -57.52 (±16.66) | -64.29* (±11.34) | -72.43 (±20.13) |
| Max_ ULD(+)/RAD | 11.57* (±21.00) | -3.62 (±29.76) | -0.32*¶ (±25.12) | -18.46¶ (±21.84) |
| Min_ ULD(+)/RAD | -8.54*¶ (±20.16) | -30.97¶ (±24.00) | -26.86*¶ (±26.26) | -46.07¶ (±23.78) |
| Max=Maximum, Min=Minimum, POE=plane of elevation, ELE=elevation, AXR=axial rotation, IR=internal roation, ER=external rotation, FLEX=flexion, EXT=extension, ULD=ulnar deviation, RAD=radial deviation * significant difference in trailing arm between side and diagonal approaches, p < 0.05 † significant difference in leading arm between side and diagonal approaches, p < 0.05 ¶ significant difference between trailing and leading arms, p < 0.05 | ||||
|
Side approach |
Diagonal approach |
||||
| Unit: Degree ( |
Trailing arm(Right) | Leading arm(Left) | Trailing arm(Right) | Leading arm(Left) | ||
Shoulder |
|
|
|
|
||
| POE_ROM | 54.84* (±24.51) | 47.88 (±11.56) | 73.76* (±20.89) | 62.56 (±18.83) | ||
| ELE_ROM | 51.90 (±19.25) | 56.05 (±16.35) | 53.57 (±27.50) | 56.87 (±18.52) | ||
| AXR_ROM | 40.21 (±11.88) | 47.28 (±10.15) | 42.66 (±13.01) | 49.66 (±6.62) | ||
| Elbow | ||||||
| FLEX/EXT ROM | 51.86*¶ (±13.71) | 34.24¶ (±14.16) | 43.31* (±9.24) | 35.70 (±7.26) | ||
| Wrist | ||||||
| FLEX/EXT ROM | 32.78¶ (±6.98) | 53.91¶ (±11.17) | 40.00 (±9.84) | 66.81 (±19.50) | ||
| ULD/RAD ROM | 20.10*¶ (±5.10) | 27.31¶ (±8.89) | 26.38* (±9.30) | 27.98 (±6.82) | ||
| Trunk | ||||||
| EXT/FLEX ROM | 36.44±5.24* 40.00±8.53 38.59±23.23* | 48.59±11.66* 44.08±9.34 56.04±29.19* | ||||
| R/L SB ROM | ||||||
| L/R AXR ROM | ||||||
| ROM=range of motion, POE=plane of elevation, ELE=elevation, AXR=axial rotation, IR=internal roation, ER=external rotation, FLEX=flexion, EXT=extension, ULD=ulnar deviation, RAD=radial deviation, R/L=right/left, SB=side bending * significant difference (in trailing arm) between side and diagonal approaches, p < 0.05 ¶ significant difference between trailing and leading arms, p < 0.05 | ||||||
DISCUSSION
The diagonal commode transfer had significantly larger shoulder forward flexion peak angle, elbow flexion peak angle, and wrist extension and radial deviation peak angles in the trailing arm, sometimes even in leading arm, than side approach. Also, they had larger shoulder and wrist ROM in trailing arm, as well as trunk ROM in flexion/extension and axial rotation during the diagonal commode transfers. These results may be due to the setup of diagonal transfers. There is a larger angle (about 108°) between the wheelchair and the commode in the diagonal approach. Thus, they used their trunk and shoulder more to cover the increased arc distance between the wheelchair and commode. The larger ranges of motions may potentially increase the risk of falling during transfers.
In the side approach, subjects used more elbow extension and less trunk and shoulder movement to perform the same transfer. Because the strategy necessitated a more trunk upright position more elbow extension was needed to elevate the hips and transfer to the commode. We found this strategy previously imparts more superior force through the shoulders, elbows, and wrists which may result in shoulder impingement syndrome, elbow injuries and exacerbate carpal tunnel syndrome. (Gagnon, Koontz, Mulroy, et al., 2009; Gagnon, Nadeau, Noreau, Dehail, & Piotte, 2008; Koontz, Kankipati, Lin, Cooper, & Boninger, 2011a, 2011b) . Although the diagonal approach required more range of motion, using more trunk flexion/extension helps to recruit larger muscle groups around the shoulder to transfer and may prevent smaller muscle groups (e.g. rotator cuff muscles) from injuries (Koontz, Kankipati, et al., 2011b) . In summary the side approach may offer greater protection from falls because less transfer distance is required, but it may result in higher superior forces and increased risk for shoulder injuries. Thus the type of transfer approach can be seen as a trade-off issue for wheelchair users. The approach chosen should match the users’ capabilities and limitations when space allows. For example, someone with weak triceps may opt for a diagonal approach because less elbow extension is needed.
Our results also show that the movement patterns between trailing and leading arms are not symmetrical in the two commode transfer approaches. In sitting pivot transfers, the upper extremities need to support about 70% of body weight (Gagnon, Nadeau, Noreau, Dehail, & Gravel, 2008), and the trailing hand sustains more peak vertical and horizontal reaction force (44.5% and 10.2% of body weight) than the leading hand (40% and 8.8% of body weight) (Gagnon, Nadeau, Noreau, Dehail, & Gravel, 2008). Future studies need to look at the forces involved when the range of motion peaks at each joint to understand more clearly the injury risks that each approach carries. Also its generally good practice to vary which arm leads to balance the loading (Boninger, et al., 2005).
Normal wrist anatomical angles for flexion, extension, radial and ulnar deviation are 60-80°, 60-75°, 20-25°, and 30-39° respectively (Norkin & White, 2009). Based on the results in the current study, the leading side wrists for the diagonal transfers experience extraneous extension and radial deviation for the diagonal transfers. These extreme wrist angles during transfers may perpetuate the development of carpal tunnel syndrome which is commonly reported among wheelchair users (Sie, Waters, Adkins, & Gellman, 1992).
The novelty of the experimental setup may have influenced the subjects’ normal transfer pattern however people generally learn to be flexible with adapting to different setups when they are out in public areas. For the same reason we don't feel that having to perform the transfers in one direction is limiting because in prior work we found no differences in muscle demands based on preferred direction of transfer (Gagnon, Koontz, Brindle, Boninger, & Cooper, 2009). This current study only looked at transfers from the wheelchair to the commode. It's likely that the movement patterns will be different for the transfer back. Future studies will entail combining the kinematics data with force data to describe the differences in joint loading between the two transfer approaches for both wheelchair to commode and commode back to wheelchair.
CONCLUSION
The wheelchair approach used for commode transfers is a tradeoff issue for wheelchair users. The side approach requires less shoulder range of motion, especially in the trailing arm, and trunk movement. Wheelchair users may be at less risk for falling during transfer because the arc distance moved through is less, but arm is positioned in a way that may sustain higher superior forces in each joint. The diagonal approach requires larger trunk movements which helps to offload shoulder forces but may carry a higher injury risk to the wrists and fall risk due to the larger degree of distance travelled. These tradeoffs should be taught to wheelchair users when they are learning how to transfer to commodes. Modifying the clear space recommendations in the ADA so both types of transfer approaches could be used would be more accommodating for wheelchair users who independently transfer.ACKNOWLEDGEMENT
This material is based upon work supported by the Department of Veterans Affairs (B7149I) and Department of Education, NIDRR (H133N110011).
The contents of this paper do not represent the views of the Department of Veterans Affairs or the United States Government.